Why researchers get it wrong
If you read any NICE guidance they always trot out the same lines about “patient centred care” and then review the evidence that is deemed high quality (RCT’s and systematic reviews/meta analysis) and then produce recommendations from that.
The issue in my opinion is that:
– They are missing out of lots of good evidence because it is not deemed of a high enough standard (not an double blinded placebo controlled RCT) or is suggested to be at risk of a bias, though this seems to be limited to certain groups as surely wouldn’t that rule out pretty much all the research done by big pharma?
– They are using evidence that is deemed high quality on a methodological level but on a biological level the researchers simply do not understand the topic on which they are researching (this might sound far fetched but I will show you later what I mean).
That said, they do still hit the mark with some guidance.
Take B12 for example, having read the literature on vitamin B12 extensively, I can tell you they are absolutely spot on for many of their recommendations (though not all).
Example, when a patent presents with neurological symptoms of B12 deficiency, they have very clear guidance on how often the patient should receive B12 injections – remember any neurological image is permanent – B12 helps make myelin.
But the real bummer is that even when NICE nail it, sadly GP’s do not follow the guidance.
I have never, ever, seen a patient with neurological symptoms get injections every other day until there was no further improvements.
It is three times a week for two weeks and then straight to every three months, which is woefully inadequate.
Now to be fair, GP’s have probably got more guidance summaries to read than the UK government has C-19 PCR/Lateral flow test kits.
However, when friendly Chiropractors like me write to them and send highlighted sections of the guidance…..they still ignore it.
Note to reader: I very, very rarely write these days, it is a waste of my time and energy and the best you might get is a injection every two months instead of three.
Next week I’ll let you in on the clinical tip to help those patients who need more B12.
But for now lets go back to the funny idea that researchers do not understand what they research.
So here is the scenario, research comes out and says for example, vitamin D is not an effective treatment for depression.
That is the headline in the papers, possibly even the research paper title and if you read the conclusions it is deffo in there.
Now if that is as far as you go, then it’s a done deal.
But the devil is in the detail, or in this case the methodology and the results.
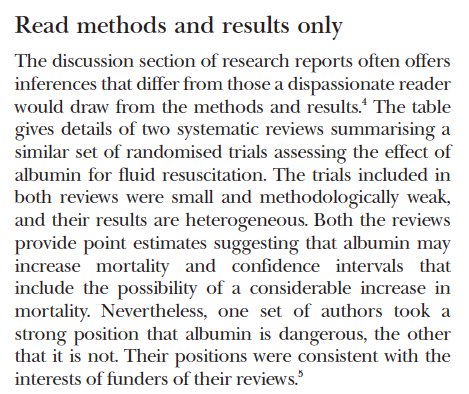
In fact if you want to detect misleading claims in research, read the methods and results and draw you own conclusions.
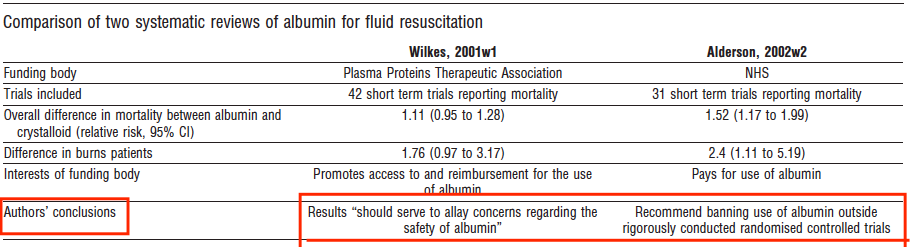
Check out the study comparison of two systematic reviews of RCT’s on the effect of albumin for fluid resuscitation. Very similar data, completely different conclusions.
So like a good little “evidenced based” practitioner you read the methods and note, they did not actually test vitamin D levels in patients, they just dished out vitamin D or a placebo.
So when they say “vitamin D is not an effective treatment for depression”, what they really mean is “vitamin D is not an effective treatment for depression in patients with unknown vitamin D status”.
But then you notice the dose……it is our old friend 400 iu (10 mcg).
Remember from the dosing chart I gave, you all have printed and laminated at clinic….right?
For every 1000iu (25 mcg) you give patients increase 25 nmol/L in blood level, see:
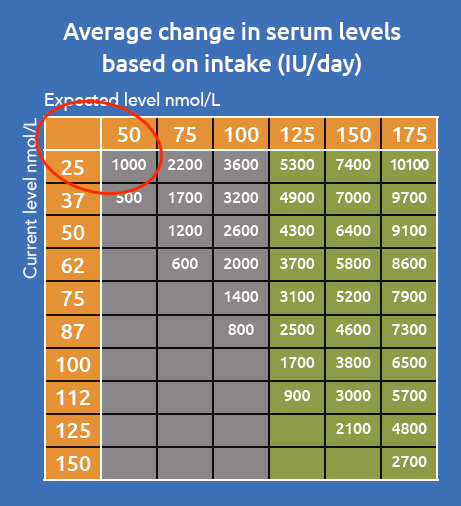
So if you were at 25 nmol/L and you took 1000 iu, you would get to 50 nmol/L.
Therefore if you give 400 iu you go up 10 nmol/L.
Now can you see the issue here of not testing?
You may have some people not deficient in the study, so they cannot benefit from the vitamin D.
And you may have some people who are deficient but they gave an dose so low it took them up 10 nmol/L but left them still in a deficient state.
Are you with me?
So the title of the paper should read “Ineffective low dose vitamin D is not an effective treatment for depression in patients with unknown vitamin D status”.
But in reality this isn’t going to get published or get any headlines, I do sometime wonder if they are designed to fail…..?
The tricky part with this is you have to really know the subject on which you are reading, otherwise you might not have the depth of knowledge to pick this stuff up.
So we could call those studies “biologically flawed”.
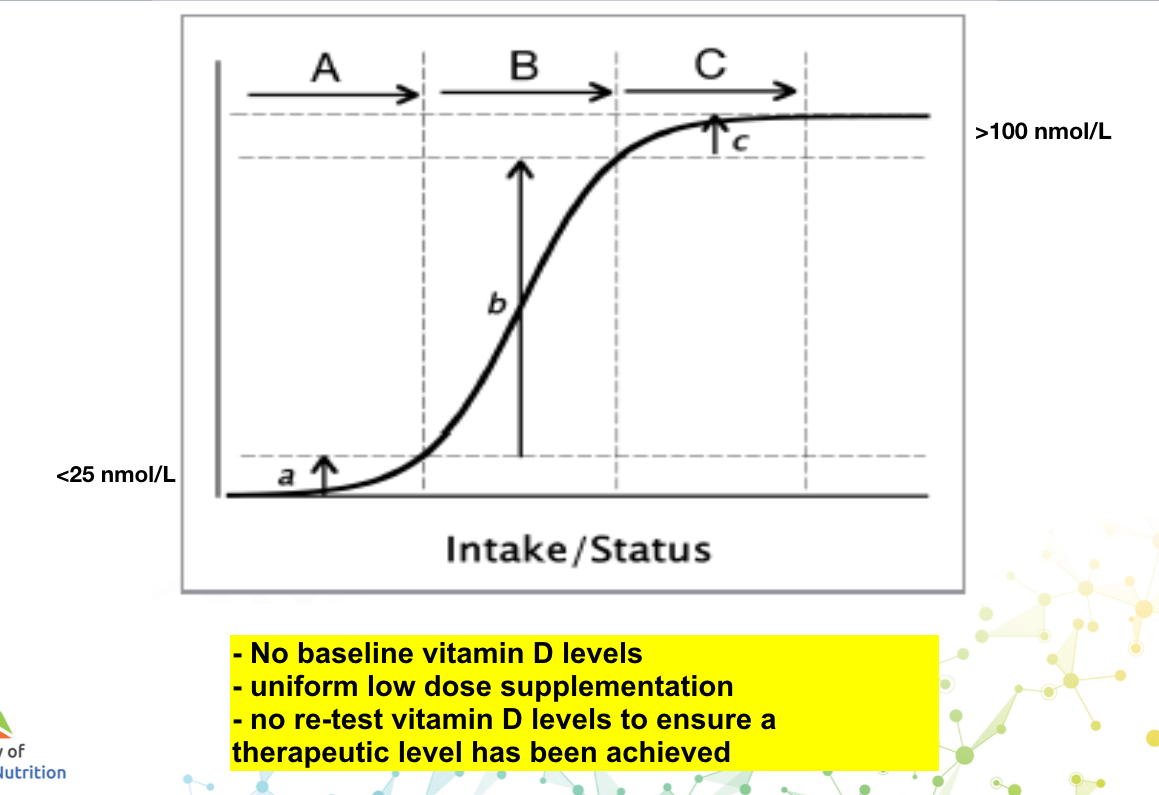
What we really need are studies that take people with known vitamin D deficiency and are dosed in personal way and re-tested to ensure they are optimal.
Then we are game on to see what the nutrient in question can do.
It is still a bit playing drugs with vitamins and it ignores the complex system that we are, with multiple other variables that might also stop the effectiveness but it’s as good as we’ll get with the current medical orthodoxy.
Now the big reveal, how did I learn this?
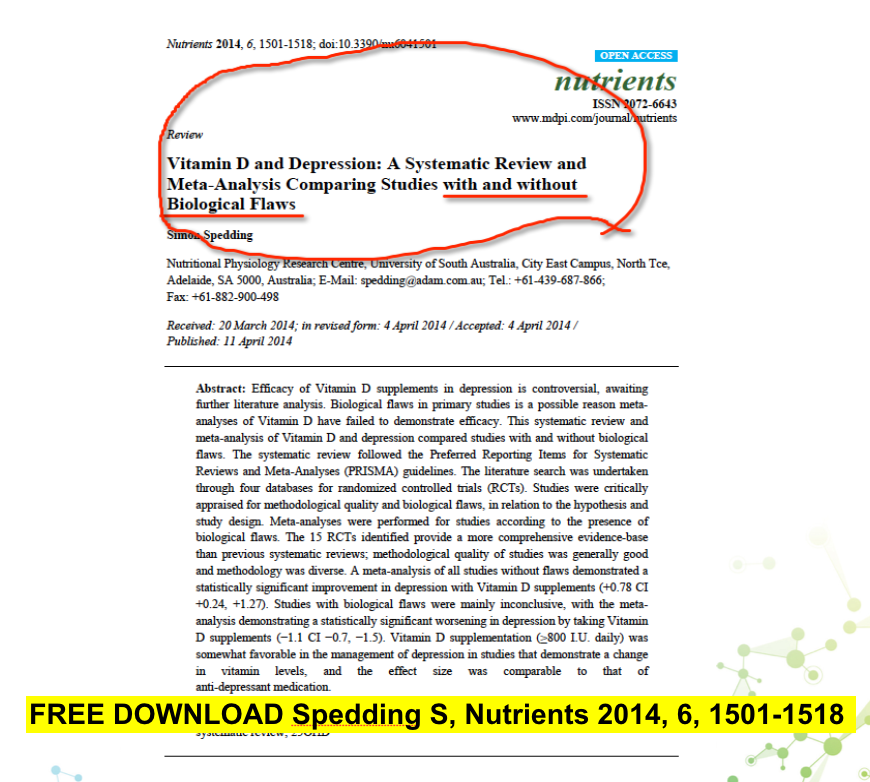
Well funny you should ask, I came across an article with that very title:
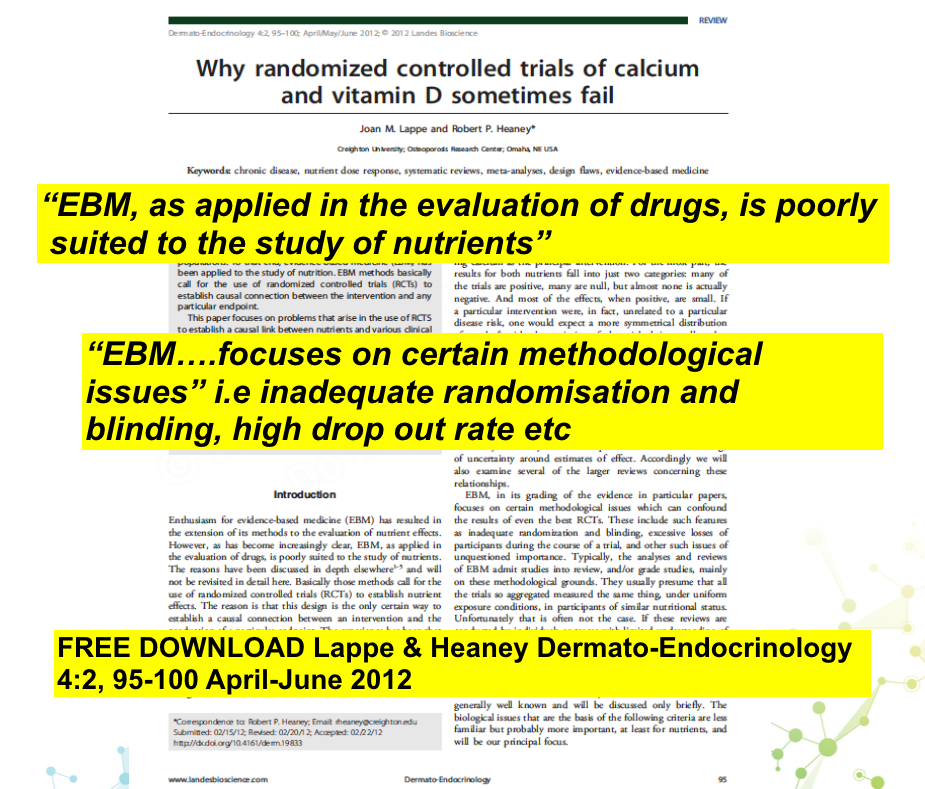
So I read it and found this article:

And then saw this diagram, which sums it up nicely.
So when we look at the conclusions of the first study we see that if they had only used studies without biological flaws vitamin D was as effective as medication.
But the studies with flaws were inconclusive or actually worse.
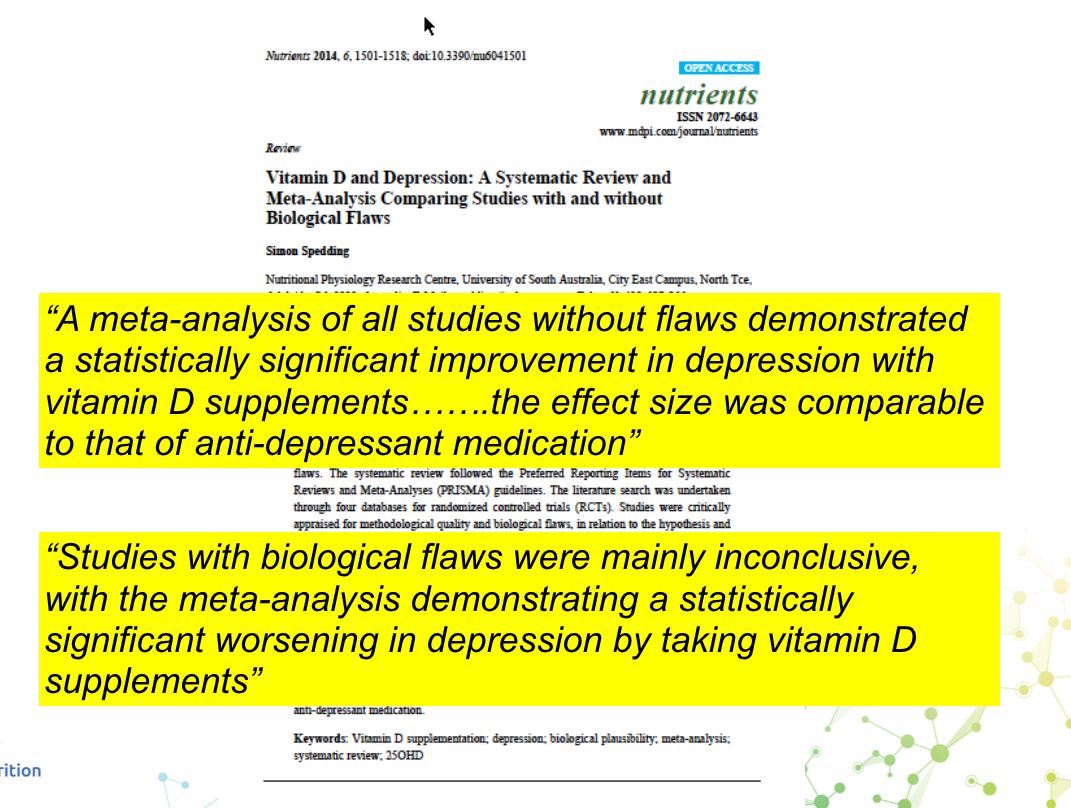
Can you see how, when the studies are then assessed in a large meta-analysis they tend to balance each other out and they find the nutrient ineffective or inconclusive in efficacy.
But we are going to be better than that, because we understand vitamin D on a biological level and we interpret the research through the lens of evolution. It is one of our:


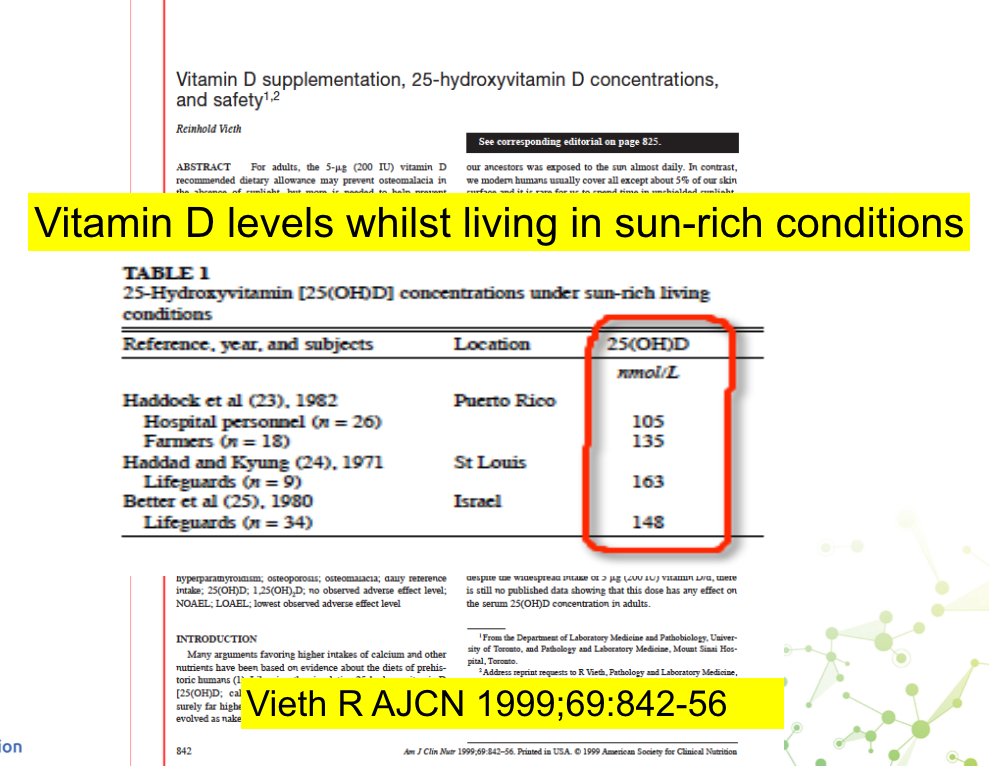
We know what levels people who live in sunny climates and work out doors have, so we want to mimic that.
Will it be a silver bullet for the patient?

Sometimes yes.
Sometimes is it one part of a larger jigsaw puzzle made from other nutritional and neuro-mechancial issues.

My job (and passion) is to read the scientific data and then make complex things simple, for you to use in clinic to get results with patients.
That is pretty much why I wrote the Core Concepts in Chiropractic Nutrition.
Then I got annoyed with sub-standard supplements and hence IN Health Supplements was born, with the formulas my patients needed, in a delivery form that works.
“The vitamin D TRAID has been a game changer for me. I usually react to supplements but the sublingual tablets have avoided any issues. I feel amazing!” – Becky Hill
Let me make you an offer…..
If you have only recently started receiving the ACN newsletter (maybe from the recent BCA webinar or word of mouth) then you can learn all about the course, see backstage and join the other members of the Core Concepts in Chiropractic Nutrition who are creating the evolution of Chiropractic, join us here:
https://www.
Remember I do the hard work for you, I read the research and tell you what you need to know to implement nutrition in clinical practice. I even have separate “nice to know” bits of the course where we get our nerd on going deep into the research that underpins the need to know information but it is your choice how deep you go.
No more watching/listening to 55 minutes of endless drivel, over endless slides of research to be given 5 minutes of useable stuff at the end.
My videos are average 10-20 minutes and I give you the good s**t at the start, keeping it clinical , all killer, no filler, my course is like a classic album.
ACTIONS TO TAKE
– When you see headlines or a article with a negative outcome, try checking the methods and if you can pick holes in it, check the results and see if the conclusions are a fair reflection of the results.
– Get your vitamin D levels tested and see where you are after a long winter