Did you see the news on chronic pain medications?
As a neuromechanical practitioner the chances are you see quite a lot of people who are in chronic pain and so the chances are you might have heard about the recent NICE guidance on chronic pain.
Nice NICE summary here ;o)…..http://www.pulsetoday.

I found the guidance and the commentary around it fascinating.
Fascinating because so much of it is so blindingly obvious to anyone who truly understands how the human body functions as a whole.
Fascinating it takes a whole committee of Doctors and researchers years of reviewing research to tell GP’s that the endless repeat prescription of opioids and NSAID’s might do patients harm.
Fascinating because they are suggesting GP’s should clearly explain the benefits and risks of the drug to the patient (the fact they are having to tell GP’s to do this should tell us something in itself).
In fairness to GP’s, they have often little else to offer via the NHS currently and as discussed before patients have completely unrealistic expectations of what the medical system can do for them.
I would not want to be a GP on the receiving end of a verbal tongue lashing from patients expecting a pill to cure them of chronic pain created by a lifetimes poor habits.
Or even worse trying to convince a patient to wean off years of 4 hourly supplies of NSAID’s and opioids.
The bottom line is the current medical model is based on an acute setting (like infection or trauma) and applying these a chronic setting works poorly.
You will be well aware that NSAID’s can cause gastric ulcers via a reduction in production of the thick gastric mucous that should stop us digesting ourselves.
The stomach (and colon) has a thick inner mucous layer and a thin outer layer. Even then with two layers the NSAID’s stop production enough that eventually the acid can create an ulcer.
However in the small intestines, the thick inner mucous is absent leaving only a thin outer layer next to the epithelium.
The reason?
You need to absorb your food into the blood to get nutrients, so it has to be thin enough to allow your broken down food to permeate the cell lining.
But the trade off is it also leaves it very vulnerable to becoming too permeable aka a “leaky gut”.
So while over a weeks, months, maybe years (maybe never) NSAID’s can reduce the gastric mucosa and help create an ulcer, in the small intestines they can induce increased permeability in 24 hours.

![]()
This means effectively the barrier between the outside and your inside (remember the gut is technically a long hollow tube running through you and isn’t technically inside you per se) is now leaky and flooding your blood stream with things that’s simply shouldn’t be there.
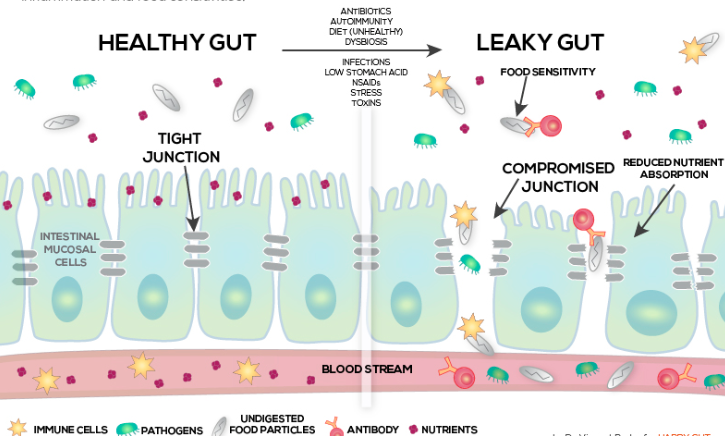
Partially digested food, pathogenic bacteria, toxins all haemorrhaging into the blood stream and the immune system recognises these should not be present and attacks accordingly.
This is why a leaky gut leads to a sustained low grade inflammatory response (response is a key word here, it is an immune response because of something or against something, it is not simply “chronic inflammation” as I was taught)
Our ancient immune system thinks we are under threat and responds in the only way it knows how.
This is the basis of food intolerances or sensitivities, immunoglobulins (IgA, IgG) targeted against food.
This all creates a vicious cycle.
Untreated neuromechanical dysfunction and connective tissue failure (macro and micro) in the presence of a sustained low grade inflammatory response (both systemically and neurologically), leads to pain, pain leads to NSAID’s, which leads to a leaky gut, which leads to more inflammation, leads to more NSAID’s/opioids/paracetamol, leads to more side-effects too numerous to discuss here, leads to more pain – repeat until they arrive at the pain clinic to be told it is “all in their head”.
In my opinion this is often best broken with metabolic intervention targeted at restoring keystone nutritional deficiencies that prime the immune system for inflammation and the nervous system for pain, plus removing the drivers of inflammation (usually food, infections and toxins) combined with high quality neuromechanical care and exercise.
ACTION TO TAKE
– Try printing the NICE guidance off and highlighting some key points for patients – they need to take ownership of their health, if it fails they are the ones to suffer.
– Encourage patients onto a modified mediterranean diet – lots of plants of different colours, high quality protein and fats, and ideally trial a removal of gluten and dairy for 2 weeks.
– Get them moving, motion is lotion and all that.