April fools medicine
Well, it has been a heck of a week here at ACN, we are loving the influx of brand new members of the evolution of neuro-mechanical care!
Remember enrolment ends tonight at midnight.
Don’t get left behind with an outdated model, a wave of health and wellness is coming and you need to integrate the metabolic world into your neuro-mechanical practice.
In other news, I am looking forward to seeing the research on cholesterol-lowering statins going on trial in the high court!!
The daily mail, vomited lies all over Dr. Malcolm Kendrick and Dr. Zoe Harcombe, accusing them of being “statin deniers”.
What is it about using the word “denier” that seems to have become so popular?
I think it might be because it suggests, without saying it, that “the science” is settled and therefore any debate (who wants that in science!) is heresy against the religion of science and medicine.
It creates a black and white view of science and research that is in reality incredibly complex.
You can read the hit job here
No surprise that the health minister at the time was happy to join in the fun.
FUN FACT: Colleagues of his gave him the nicknames, Matt Wankcock and Matt Handjob, I couldn’t agree more.
Check out the tragedy of Matt Hancock (and of British politics)

Anyhoo, when it comes to statins the main game of smoke and mirrors runs like this:
Whenever possible, only assess the reduction of one heart attack as your endpoint for success. Do not use all-cause mortality (excluding trauma) because it tends to wipe out any wafer-thin benefits.
Try to use patients with existing known heart issues in studies because you have a way better chance of stopping another heart attack in patients already known to have issues than for primary prevention. But then the data can be used to justify the treatment of patients with no known history of heart issues (primary prevention) in national guidance.
Make sure the researchers on the national guidance committee for deciding on the use of statins are mainly on the pay roll for the drug companies who make the drugs (FYI it was 8 of out 12).

That way, they can push everyone over the age of 50 to be on statins.


Mix up different ages and genders because the drug only seems to have any microscopically small benefits in males under the age of 69.
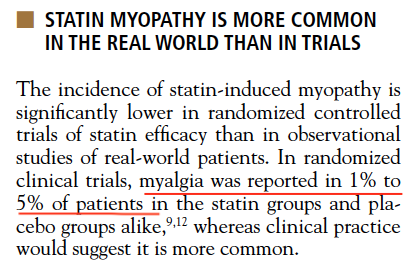
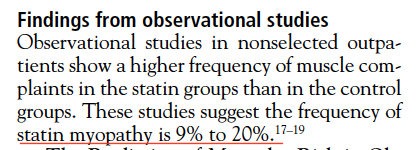
Anyone that complains of muscle pain during the run in phase of the trial, remove them, then start the trial proper. That way, you can claim the adverse event rates are 1-2 % not 20%.
Vs
Take meaningless absolute risk reductions like 1% and turn them into relative risk reductions like 33%, because a drop from 3% risk to 2% risk is RELATIVELY a drop of a third of 33%.
Example:
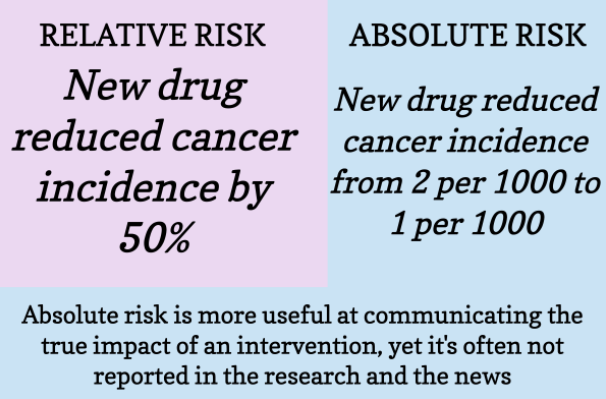
Otherwise, if you actually explain the real risk reduction/likelyhood they will benefit, they won’t take the pills!

Or you can scare people with relative risk increases.

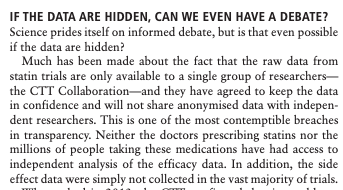
Never, ever allow independent researchers access to your raw data, ever.
Even if the editor of the BMJ and other leading independent researchers are regularly asking for it, just ignore them.

![]()
Sure, they will complain for years about the lack of transparency and how unscientific it is, but at the end of the day, they are not breaking any rules.
Make sure the conclusions section of your research paper is completely at odds with the results section to avoid any accusations that the results suggest very little benefit was achieved.
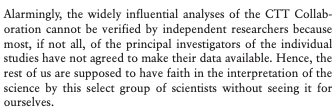
Never use statistics like the number needed to treat (NNT), it makes the drugs look completely useless, especially when it is for all-cause mortality.
If this all sounds a bit much and maybe I am over egging the medicine is corrupt cake, check out this recent opinion piece in the BMJ, called “The illusion of evidence based medicine”, catchy title isn’t it.

But what will happen in court? Will the judge allow a real dissection of the data and understand that the data is potentially bent?
It will be fascinating to see if the hallowed halls of the highest court in the land are immune to the influence of big pharma.